With more and more and people pursuing active lifestyles, hip injuries in sports have become a concern in terms of loss of time and talent. A lot of the regular people have taken up regular cycling, football, running, etc. type of sports to maintain their health and/or as a leisure sport. We have seen a rise in the cases of hip injuries in athletic as well as active individuals in the clinic, since the lockdown in March 2020 because inspite of being active the overall sitting time or time indoors was found to be a bit high.
It came to my notice that, its the end of 2022 and many of these sports enthusiaists, runners and active sports players have not been able to completely get rid of the hip injury yet, so i decided to just put up my perspective about hip injuries in various sports.
Hip injuries can really disable the injured as it may affect the daily activities as well the ability to perform the sport. Secondly, hip injuries can also be confusing, cause the injured may not experience pain directly at or around the hip, but pain can be felt at the lower back or the pelvis.
Sports that have displayed a higher prevalence of hip injuries include ballet, soccer, hockey, baseball, golf, and running. Depending on the sport, the athlete’s hip may be subjected to various extra physiological forces that are capable of causing acute or chronic injury to the hip.
To understand the hip let’s first go through the basic making of the hip joint.
Anatomy of the hip joint:-
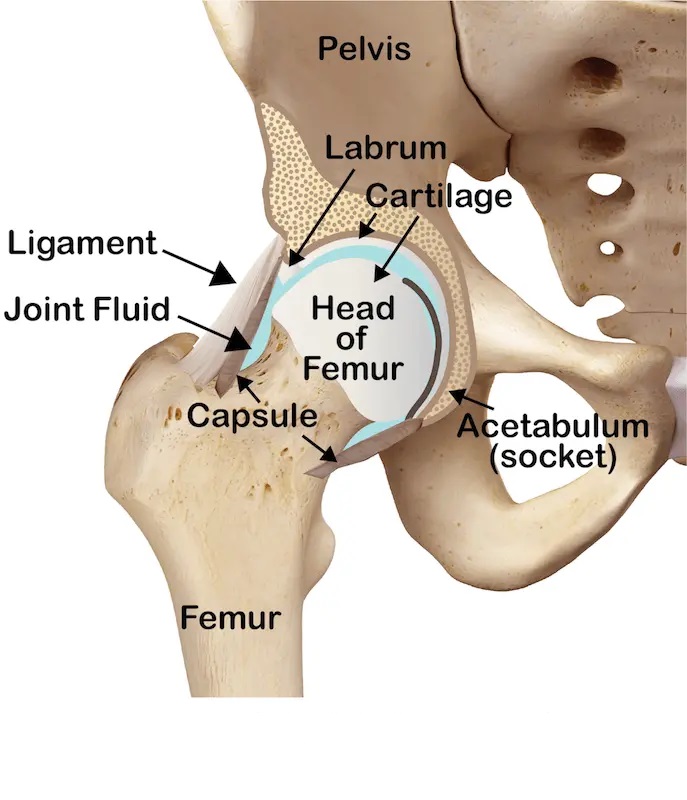
- The Hip joint is made up of two bones named femoral head and acetabulum which appear like a ball and socket.
- The depth of the socket is not enough to accommodate the larger femoral head which is why there is a fibrocartilaginous ring or labrum which deepens the acetabulum and helps to stabilize the hip joint, increasing the contact area and decreasing the joint stress.
- The labrum has some sensory nerve endings which means that any damage occurring to it will be signaled to the brain. Any tear in the labrum will lead to joint pain and destabilize the joint which will eventually contribute to increased stress on the hip joint.
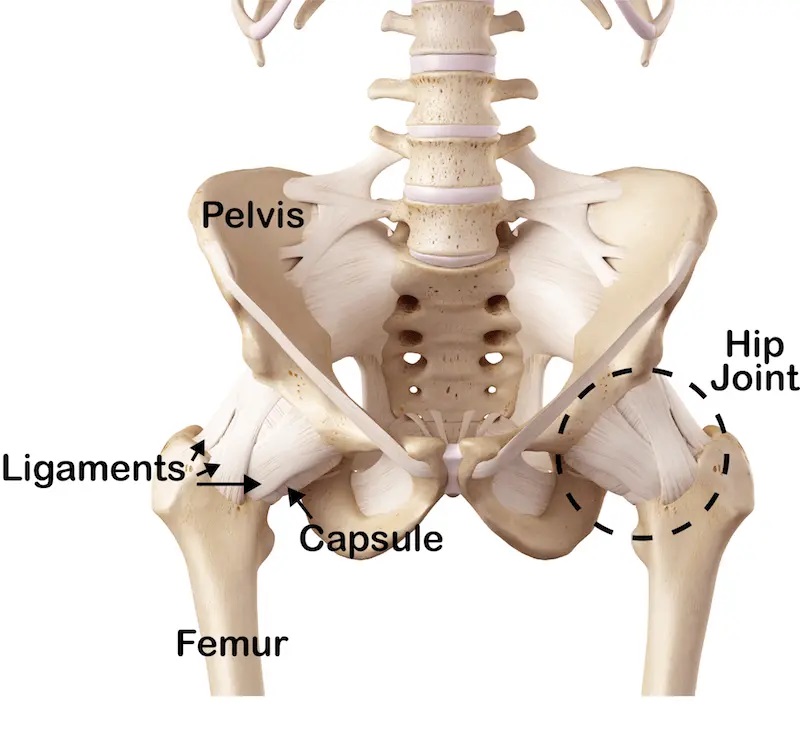
- Hip joint capsule: The hip joint capsule is strong and dense which covers the femoral head and neck like a sleeve and gives more stability to the hip joint.
- Ligaments around Hip joint: The 3 main ligaments around the hip joints are the Iliofemoral ligament, Pubofemoral ligament, and Ischiofemoral ligament which is also called the capsular ligament they reinforce the joint capsule.

- The Ilio-femoral ligament is a very strong and thick ligament situated anteriorly to the joint. It is a “Y” shaped ligament. It reinforces the capsule anteriorly to stabilize the hip joint. The
- The pubofemoral ligament connects the pubic bone to the femur bone. It strengthens the anterior and inferior aspects of the capsule
- Ischiofemoral ligament is a spiral-shaped ligament that attaches at the body of the ischium behind and below the acetabulum proximally and attaches distally at the superior part of the neck and root of the greater trochanter.
- All 3 ligaments restrict and control the different movements of the hip. The iliofemoral and pubofemoral ligaments restrict lateral rotation (outward turning) and ischiofemoral ligament restricts medial rotation (inward turning) of Hip joint.
- Blood supply to Hip joint: It receives blood supply from medial and lateral circumflex arteries, obturator arteries, and superior and inferior gluteal arteries
- Nerve supply: The nerve supply to the hip joint is from the femoral and obturator nerves from the Lumbar plexus and the superior gluteal nerve and the nerve to quadrates femoris from the Sacral plexus.
- Muscles around hip joint:

- Hip flexors: the primary hip flexors are Ilio-psoas, rectus femoris, tensor fascia lata, and Sartorius
- Hip extensors: the hip extensors are one joint gluteus maximus muscle and two joint hamstring muscle
- Abductors: The primary hip abductors are the gluteus medius and gluteus minimus and secondary muscles are ITB and TFL.
- Adductors: the adductors of the hip are Pectineus, Adductor longus, adductor brevis, adductor magnus, and gracilis Lateral rotators: Obturator internus and externus, gammellus superior and inferior, quadratus femoris and piriformis Medial rotators: Anterior portions of Gluteus medius and TFL.
Causes of Hip Injuries in Sports:-
Causes can be intrinsic ( that is due to faults in the shape of the bones or tight or loose muscles) or they can be extrinsic ( from factors which are related to your work or sport and affect our hip joint structures).
In this section we will elaborate on the cause of the hip Injuries sportwise:
Hip Injuries in Cyclists: –
For a regular cyclist or a triathlete reading this, you must know that the hip will work the most while you are cycling and even when you are not.
Normally biomechanical overloading of the hip joint causes more injuries than direct trauma.
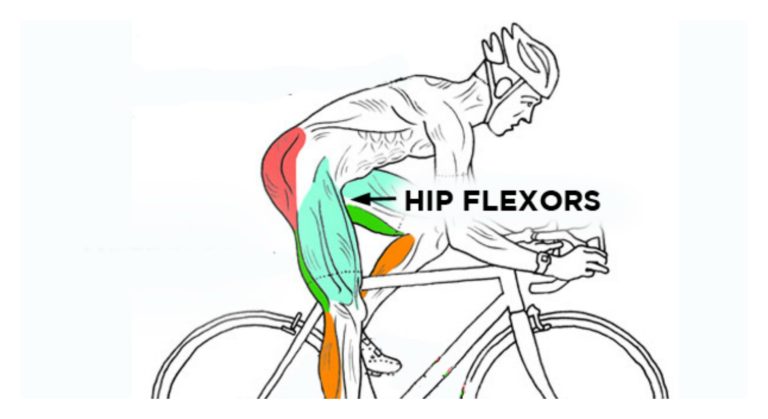 for example, the action of cycling involves repeated hip flexion with the hip never full extending, which can cause tightness or even a shortening of the hip flexor muscle over time. Prolonged periods of time sitting also contribute to tight hip flexors, such as time spent at a desk or driving. so it very common for cyclists with hip/lower back injuries to have tight hip flexors
for example, the action of cycling involves repeated hip flexion with the hip never full extending, which can cause tightness or even a shortening of the hip flexor muscle over time. Prolonged periods of time sitting also contribute to tight hip flexors, such as time spent at a desk or driving. so it very common for cyclists with hip/lower back injuries to have tight hip flexors
 It’s also known that a poor bike fit puts all the wrong pressure in the saddle area which in combination with intrinsic factors like poor flexibility and or faulty leg alignment while cycling leads to most hip injuries. A poor bike fit can also cause tendinopathies in the hamstrings as well as the hip flexor tendons.
It’s also known that a poor bike fit puts all the wrong pressure in the saddle area which in combination with intrinsic factors like poor flexibility and or faulty leg alignment while cycling leads to most hip injuries. A poor bike fit can also cause tendinopathies in the hamstrings as well as the hip flexor tendons.
moreover, a poor bike fit can worsen the already existing arthritis, as the cyclists might have to flex it beyond the available range. Leading to more strain and worsening of the inflammation in the hip joint.
overtraining or incorrect seat height can fire up the iliotibial band. It is often accompanied by trochanteric bursitis and is characterized by pain and point tenderness over the greater trochanter. In some cases, crepitus or clicking may be audible. Iliotibial band syndrome can also produce symptoms at the knee joint or its insertion site on the tibia. Signs and symptoms include pain with motion at the lateral femoral epicondyle or Gerdy’s tubercle.
Hip Injuries in Running:
 One of scariest cases in the clinic was a 50-year-old female runner diagnosed with stress fracture while she was training for her full marathon. Sadly, she never completed the full marathon but here is a list of reasons why you may get a hip injury while running.
One of scariest cases in the clinic was a 50-year-old female runner diagnosed with stress fracture while she was training for her full marathon. Sadly, she never completed the full marathon but here is a list of reasons why you may get a hip injury while running.
Hip injuries in runners are due to interactions of intrinsic and extrinsic factors that adversely affect the complex regional anatomy. acute or chronic hip pain are a challenge to diagnose as the symptoms are vague and may arise from parts of the body other than the hip.
Most running-related injuries affecting the lower extremities are due to preventable training errors, and some may necessitate medical evaluation or a significant reduction in training.
what we have seen is that less experienced runners and runners with higher body mass index, end up being more prone to injuries in general.
Strong evidence that found that previous or existing lower body running injury can cause a new or the same injury again. Hence we have so many clients who keep getting IT band-related issues again and again until they complete the rehab pin to post.
Apophysitis and avulsion fractures may affect younger runners and produce localized pain at muscle attachment sites.
Stress fractures are potentially serious conditions that affect women more frequently than men. They are more common in females due to a wider pelvis which places the body weight at a different angle compared to men with a narrow pelvis.
While running at each step there is a point where each leg bears the weight of the whole body while the other leg is in the air. If there is a lack of mobility, then the muscles supporting the hip will restrict the movement of the joint leading to more strain in each step you run. if there is a lack of stability then muscles supposed to be working will not come into action leading to pressure on the stance leg, which may lead to various running injuries of the hip.
Muscle strains and tendonitis are the most common causes of hip pain and typically result from sudden increase/decrease of speed while running, direction changes, or eccentric contractions.
Hip Injuries in Football: –
Usually, hip injuries are more common in two muscles in footballers. Namely
- Iliopsoas. (hip flexor)
- Adductors. (groin muscles)
The most common mechanism is sprinting, kicking, and change in directions. Adductor and psoas strains are typically noncontact injuries and usually result from eccentric loading when attempting to kick a ball. eccentric load means the muscle is loaded when it is in a stretched position.
In my experience, I have seen hip injuries occur usually due to: –
- shooting practices where the player takes multiple kicks.
- Goalie practices where the goalkeeper rehearses goal kicks or punts over and over.
- repetitive sprint training
- no proper rest in between back-to-back games.
- improper rest and early return to sport in a previous muscle strain injury.
We have also conducted pre-season musculoskeletal check-ups for a football team. And as per our understanding.
- A measure of total hip rotation less than 85 degrees – means the hip mobility is on the lesser side and the chances of injuries higher. So we always add a few hip mobility drills for such a player.
- Low strength ratios of inner thigh muscle compared to outer thigh muscles, means the overall stability of the hip is compromised and chances of getting the hip injury are higher.
- As per research, differences have been identified in the star excursion balance test of posterolateral reach and altered intersegmental biomechanics in various cutting tasks in those with HAGI (hip and groin injury). This means while testing the star excursion balance test if the player has a weaker posterolateral reach, he or she is more susceptible to hip injuries.
Hip impingement is also one of the common injuries affecting footballers. Sometimes the cause of such injuries can also be the shape of the pelvic bones. Research conducted on soccer players with hip pain noted that a faulty shape of the iliac bone leads to impingements in soccer players.
Both type II and III morphologic variations decrease the space available for soft tissue recoil and may cause mechanical impingement of hip motion (mainly hip flexion and internal rotation)
Hip Injuries in Dancers: –
Dancers move various body segments in a repetitive rhythmic fashion to demonstrate their artistic expression and athletic prowess while placing significant physical demands on their bodies. This often requires extreme ranges of motion, particularly of the hip, as well as controlled displays of strength to obtain optimal form.
While professional dancers were more prone to hip/groin injuries than their student counterparts, the etiology is unclear: It may be secondary to higher levels of training or skill, increased exposure time, or older age. As a group, professional dancers tend to be older, with hip injuries in dancers occurring with increasing age.
Dance injuries can be classified as either traumatic or overuse, a factor considered in 3 studies presented. Not surprisingly, given the repetitive nature and extreme ranges of motion required in dance, overuse injuries of the hip are more common than acute traumatic injuries among dancers.
Hip and groin injuries are an important health issue for dancers of all skill levels, presenting with an injury rate of 17.7% in this systematic review.
Research has also shown snapping of the hip flexor as the highest occurrence among dancers followed by snapping of the hamstring tendon due to moves requiring extreme ranges.
Hip Injuries in Cricket
Hip injuries in cricket are rarely reported often at a professional level. There is no research which talks about them but they are happening in less experienced and adolescent cricketers.
There are researches done, which state that women cricketers with lesser neuromuscular control are susceptible to injuries but they do not specify only hip injuries, they can be in the lower back/groin/knee/ankle.
 In my personal experience of working with adolescent cricketers, I feel that a weakness in the lower body chain which must activate during the bowling or batting action can become a cause for a hip injury. For example, for a fast bowler, chances of hip injuries are higher due to faulty landing on the pitch or improper run-up to take a jump while bowling.
In my personal experience of working with adolescent cricketers, I feel that a weakness in the lower body chain which must activate during the bowling or batting action can become a cause for a hip injury. For example, for a fast bowler, chances of hip injuries are higher due to faulty landing on the pitch or improper run-up to take a jump while bowling.
Mainly, female cricketers who are training to be better fast bowlers and have to change their bowling style every other season may be a party to a hip injury. In addition to that, when the foot lands for bowling there is a force pushing the knee inward called the knee valgus force. Say if the cricketer has poor neuromuscular control or balance, the feedforward mechanisms of the muscle chain are delayed to prevent this force and the hip or back muscles may not support the knee landing….leading to wear and tear, which may trigger early arthritic changes in the hip.
Common Hip Injuries in sports: –
-
- Muscle strain and tendinopathies:- common muscle strains in the hip area on the hip flexor tendon (iliopsoas strains), inner thigh muscles ( adductor strains), upper hamstrings strain, piriformis strain and last is the buttock muscles (gluteus medius tendinopathies) at the greater trochanter. They can range from a minor strain that recovers in 2 to 4 weeks to complete tear which required 12 weeks minimum to recover, or they can be due to the irritation of the tendon at the site of insertion.
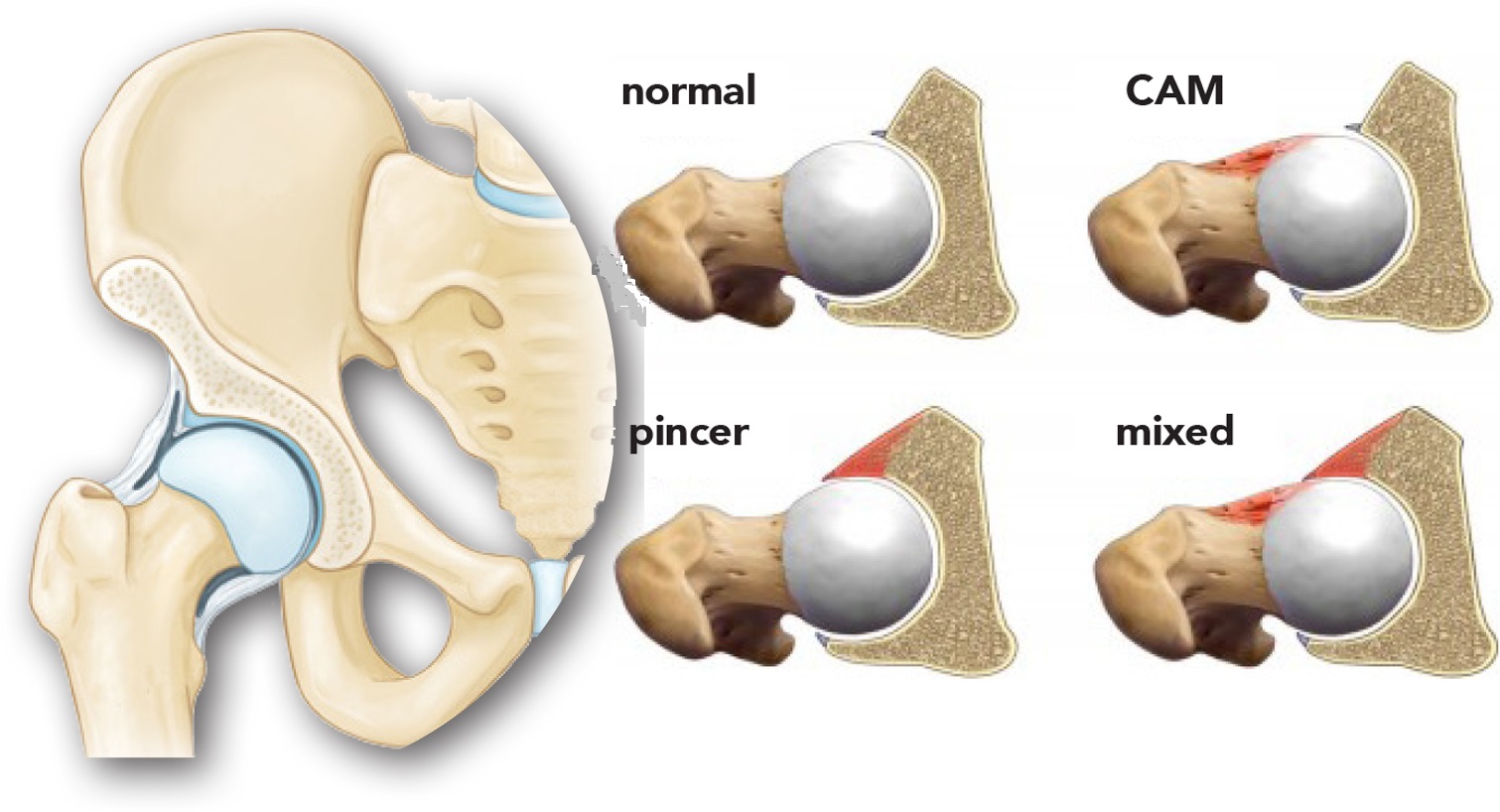
- Hip impingement:
 Impingement means that the space between the two bones has decreased either due to overgrowth/ undergrowth of one bone which causes pain with movement as the bone doesn’t have enough space to move leading to increased stress. Impingement also leads to grinding of the cartilage and the labrum in that area.
Impingement means that the space between the two bones has decreased either due to overgrowth/ undergrowth of one bone which causes pain with movement as the bone doesn’t have enough space to move leading to increased stress. Impingement also leads to grinding of the cartilage and the labrum in that area. - Bursitis of the hip joint: – bursitis in the hip means swollen fluid sac located on the outer side of the hip at a bony prominence called the greater trochanter. 2 of the buttock muscles come and insert on the GT. There is usually pain at the outer side of the hip with walking, climbing stairs, running, getting in and out of the car.
- Labral tear in the hip: labral tears can occur in any age group, but mostly affects young active adults and females more than males. Labral tears occur due to repeated microtrauma from twisting motions. Labral tears if left untreated may lead to degenerative changes in the hip joint.
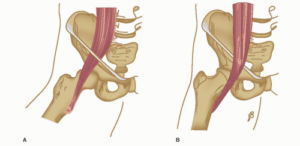
- Adolescent hip injuries: The incidence of avulsion fractures is increasing, among teenage athletes because of the growth in competitive sports participation. Avulsion injuries are common among skeletally immature athletes due to the weakness across the open apophysis. It is mainly caused by sudden, violent, or unbalanced muscle contraction, and are common in sports such as soccer, ice hockey, gymnastics, and sprinting, which involve kicking, rapid acceleration and deceleration, and jumping
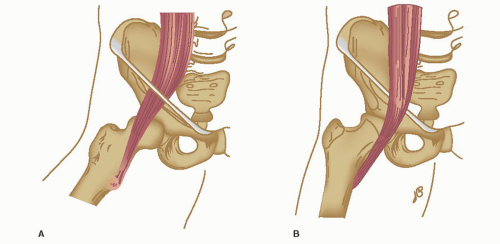
- Snapping hip syndrome: It’s is a symptom complex characterized by pain and an audible or perceived snapping of the hip during movements. Snapping hip (also known as coxa saltans)may be the result of intraarticular (within the hip joint), extra-articular (outside the joint) pathology.
In cases of external coxa saltans, the history can be extremely helpful in establishing the diagnosis. Patients will explain a “snapping, painful” sensation over the lateral hip and commonly localize pain to the greater trochanter when asked to identify the area of maximal tenderness. Traditionally, the external snapping hip has been associated with a thickened posterior border of the iliotibial (IT) band or anterior border of the gluteus maximus, which predisposes the IT band to slip back and forth over the greater trochanter. The thickened IT band lies posterior to the greater trochanter as the hip sits in extension, and as the hip is flexed, the band forcefully slides anteriorly over the trochanter, producing pain and an audible sound. The greater trochanteric bursa, which lies between the IT band and the greater trochanter, can become inflamed as the band continuously slides over the bursa, leading to inflammation and contributing to the patient’s painful symptoms.
Patients with internal coxa saltans typically describe a painful clicking/popping sensation emanating from the deep, anterior groin. It is now well accepted that the source of pain and audible snapping is produced by subluxation of the iliopsoas tendon during hip range of motion.
- Hip cartilage injuries: Chondral injuries are wear and tear of the cartilage in the hip joint that can occur in association with labral tears,femoroacetabular impingement, posterior dislocation,dysplasia, and osteoarthritis and can lead to cartilage erosions, deformity of the femoral head, and loose bodies.
- Stress fracture of the hip joint:- stress fractures occur usually in bones that are fatigued. They are also called fatigue fractures. In active population, usually, stress fracture will develop as microfractures that don’t get a chance to heal because there is a small amount of bearable load being put on the hip continously. Additionally, if there is an imbalance between bone resorption and bone formation, then the chances of stress fractures are high.
- Inflamed /Arthritic hip joint:- developing wear and tear in the hip is a known fact, but pursuing an active lifestyle with the arthritic hip can be tricky. If the joint is not taken care of while playing the sport, the inflammation may get worse and cause more arthritis. Hip osteoarthritis may also produce persistent pain that worsens with running.
Examination of hip injuries:-
Examination starts from the point the client walks in….
- We check the walking pattern as the client walks in
- A detailed history is recorded to understand how the injury occurred
- The normal body movements are tested in standing as well as lying down.
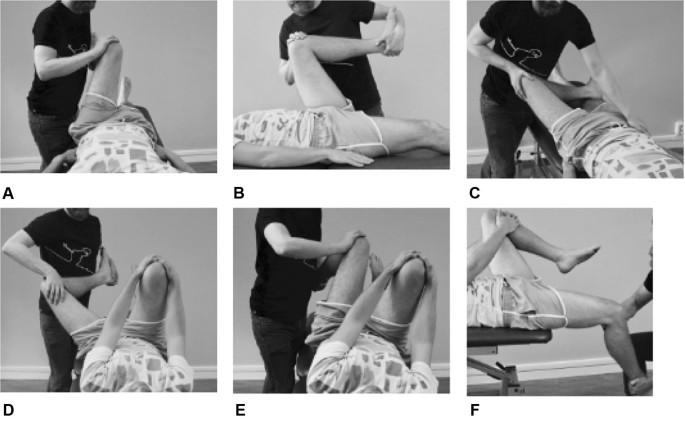
- Special tests to reach a diagnosis are done. Tests like FABER, FADIR, muscle strain tests, Trendelenburg’s test, leg length discrepancy test, squeeze test, etc. are done only if the client is pain-free and able to bear the strain.
- Also, functional movements are examined to test, if the client is able to do sit to stand, stairs, walk-run, squat assessment, or a particular sport-specific action is tested to see if it aggravates the pain.
- For sports-related injuries, mobility and stability movements are also tested to understand the movement deficiencies.
- The ergonomic assessment for work-related hip injury is also discussed.
- Nevertheless, we check the entire lower back, the knee as well as ankle for any restrictions to design an appropriate rehab program.
Clinical presentation
- Altered walking/ running pattern. Have u seen a runner limp while running?
- Change in weight-bearing status on the injured side maybe there while performing exercise or sports.
- Restricted movements of the hip in all or some directions
- Altered length of the muscles- they may be tight or too elongated. For example, if the muscle is elongated then you might have difficulty controlling that particular hip movement but if it is tight you might not be able to perform that particular hip movement)
- Altered / faulty posture of the lower extremity. For example, If you have knock knees then your hip bone may be turned inward as a structural or a functional deformity which means the posture is faulty at the hip level too.
- Pain may be dull aching, widespread (that is your lower back or knee or ankle may hurt as well), or it may be sharp shooting pain in certain positions or activities only.
Management of Hip Injuries in Sports:-
Management of hip injuries is complex but simple. We believe in treating the client as a whole and not looking at the problem from just one single joint injury perspective. The goals of managing hip injuries in sports or regular individuals’ via physiotherapy are
- To improve the range of motion
- To reduce pain
- To improve the strength of the hip muscles and the muscles in the chain (lower back, knee, ankle, core strength)
- To improve the functional movements (walking climbing, sitting for regular individuals and sports-based movements for athletes)
- To educate the client regarding the injury and motivate them to follow the rehab till the end.
There are some facts, which the researchers have been able to verify in regards to multiple aspects of physiotherapy management for hip injuries in sports as well as regular people. They are:-
- Physiotherapy rehabilitation costs lesser than surgical management in the case of FAI (hip impingement).
- Physiotherapy treatment which includes manual therapy plus hip strengthening for 3 months had better outcomes for hip OA compared to surgical management.
- Sports injuries like FAI are well managed via physiotherapy compared to arthroscopy. But the return to sport varied up to 16+ months whether the client was managed surgically or with physio alone. Hence researchers have quoted “ Arthroscopic surgery could be recommended as a second-line treatment for patients who have not responded adequately to a physiotherapist-led treatment program.“
- For hip pain, the research claims that physiotherapy treatment is more effective in a span of 3 months, but the researchers are not sure about the quality of life improvement. Secondly, the research also claims that post hip arthroscopy for hip pain, there was small positive improvement at 8 to 9 months.
Physiotherapist-led interventions on physical impairments had variable effects. For hip range of motion, the largest positive effects pre-physiotherapist-led to post-physiotherapist-led treatment were seen following a 3-month intervention strengthening exercise, manual therapy and education.40 The greatest hip muscle strength gain was seen with a strengthening exercise programme of 3 months duration,40 and largest in hip adductor muscles. Greater hip adductor strength following hip arthroscopy is associated with better hip-related QOL,46 suggesting that it may be an important target.
- Research also says that most people who opt for early surgery are teenagers or young adults who want an early return to sports. But however, the return to sport time remains the same with or without the surgery.
Returning to pre-injury sport and activity is important to young and middle-aged people with hip pain, and often the reason they seek surgical and/or non-surgical treatment.However, only two studies in this review had a specific return to sport/return to physical activity component within the physiotherapist-led intervention.Only 17% of people returned to optimal performance and full sports participation at 33±16 months following hip arthroscopy. Given the importance of returning to sport in this active patient group and the disappointing rates of returning to optimal performance reported,future studies should incorporate key functional and sporting components.
Our hip injury management style: –
- On the first day of the clinic visit mainly the symptoms which are aggravating the pain are addressed via manual therapy or electrotherapy and exercises.
- A rehab program is devised customizing the client’s sporting needs. For example, a runner with hip injuries will be given a progressive rehab program close to a running pattern.
- Pain is usually addressed via various manual therapy techniques, dry needling, electrotherapy, and supportive taping.
- We also provide advice for certain do’s and don’ts to deal with hip injuries. The ergonomics of the work setup is assessed and corrections regarding seating position are advised.
- For sports injuries, we usually connect to the trainer and coaches and make necessary adjustments in the players playing style to prevent the re-injury.
- The treatment program usually lasts between 8 weeks to 6 months wherein the client is usually called for follow-ups and is expected to follow the rehab back at home. Return to sport usually takes 9+ months depending on the severity of the injury and individual factors.
- Last but not the least, we believe in educating the client regarding the injury and motivating them to follow the rehab till the end.
here is a list of 9 simple exercises to relieve your hip pain.
References:-
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4767832/
- https://cme.lww.com/files/-1519830203420.pdf
- https://www.jorgechahlamd.com/wp-content/uploads/2020/12/232-Hip-Injuries-Kicking-Athletes.pdf
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4338213/
- https://link.springer.com/article/10.2165/00007256-200535110-00005
- https://bjsm.bmj.com/content/54/23/1382
contact us:-
feel free to contact us via following links
https://g.page/r/CXbQDl0Agna9EAE
https://www.instagram.com/physiocure/?hl=en