After coming across the normal thought process of most patients visiting our clinic, we decided to put forward a small write up to make a layman understand that “not all shoulder pains are frozen shoulders”.
It is estimated that 30% of people will experience shoulder pain sometime during life (Lewis 2009b, p. 259). ‘The incidence of shoulder pain increases substantially with age, and for people over 65 years of age shoulder pain is the most common musculoskeletal problem’ (Taylor 2005, cited in Lewis 2009a, p. 236).
Shoulder pains can be classified into variety of different diagnoses like Sub acromial Impingement, Rotator cuff syndrome, Cervical radiculopathy, AC joint strain/arthritis and many more. In this article we will be discussing about the Sub Acromial impingement Syndrome(SAIS).

WHAT IS IMPINGEMENT?
Shoulder muscles get pinched between the bones that form your shoulder leading to shoulder pain. This is medically diagnosed as an Impingement. This impingement can be due to structural faults in the bones or tendons or muscles or due to faulty biomechanics .
To understand the above medical diagnoses let us first understand the anatomy and the factors which cause this kind of pain.
ANATOMY AND BIOMECHANICS OF SUB ACROMIAL AREA:-
The shoulder joint:-
This joint is formed of 3 bones namely the humerus or the arm bone, the clavicle or the collar bone and the scapula or the shoulder blade bone. There are total 4 joints between these bones and your rib cage which form the shoulder namely
- Glenohumeral joint( GHJ) connecting the arm bone, collar bone and shoulder blade at the corner of your shoulder;
- Coracoacromial joint( CAJ) between the collar bone and the shoulder blade;
- Scapulothoracic joint (SCJ) between the rib cage and the shoulder blade and
- Acromioclavicular (ACJ) joint between the shoulder blade and collar bone again.
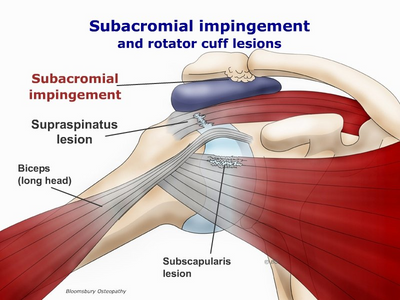
Other than these 4 joints, ti Understand SAIS, we need to understand the area at the tip of the shoulder formed by the GHJ & the ACJ, called the Subacromial area. Other than bones it has a bursa, tendon of the muscle Supraspinatus & biceps, which are mainly affected in SAIS
The subacromial bursa (SAB)

- A bursa is a sac filled with nourishing fluid cells and some fat tissue. It normally is present between the bones which end up forming a joint as its main role is to prevent friction between these bones. The shoulder has 7-8 bursae of which “subacromial bursa(SAB)” is the largest.
- There are a group of muscles called the rotator cuff (RC) muscles which maintain our shoulder joint compact. There many other muscles which cross the shoulder joints.
- The SAB separated the RC muscle ends which form tendons to attach on the bone from another major muscle called the deltoid.
- The SAB also separates an important ligament called the coraco acromial ligament from these muscles thereby preventing friction between these muscles and ligaments on the bone.
- The SAB has wiring as well that is nerves which cause the sensation of pain when there is something wrong with this bursa.
DIFFERENT CAUSES OF CHRONIC SHOULDER PAIN IN PEOPLE OVER 40 YEARS OLD ARE (Codsi, 2007, p. 473).
Below is a list of diagnoses which comprise a range of pathologies which can cause shoulder pain
| The common causes | Other causes of pain are:
|
Causes of referred pain:
|
|
|
|
THE PATHOLOGY OF SAIS:-
Impingement syndrome is a generic term used to describe RC lesions, from early inflammation through degeneration to partial/complete tears). Number of hypotheses has been suggested for the etiology of SAIS: structural factors (like acromial shape), hypermobility and instability of the GHJ, internal impingement, capsule contraction, and RC tendinitis (Lewis, Green & Wright 2005, p. 385; Ainsworth & Lewis 2007, p. 208).
Intrinsic theories

- These theories are based on changes occurring inside the tendons of the muscles attached in this subacromial space.
- The changes occur either due to limited blood supply, constant/repetitive compression which eventually cause negative changes in the basic structure of the tendon leading to wear and tear.
- Intratendinous degeneration or tendinosis might occur as a result of the combination of limited vascularity in CODMAN’S CRITICAL ZONE and external compression of the tendon structures in the subacromial space’
- Because of these intrinsic changes within the tendon, they indirectly affect its strength. These wear and tear changes cause the tendon to develop cartilage like properties at the attachment site making them susceptible to tears which also cause changes in the shape of the bone acromion where they attach.
Extrinsic theories
- Nho et al. (2008, p. 988) suggest the influence of age and activity on the shape of the acromion, as well as environmental causes such as age, co-morbidities (like diabetes mellitus and smoking) and overuse in impairing the healing processes of the tendon.
- It seems that superior translation of the humeral head plays a significant role in the pathology (Lewis 2009a, p. 239).
- Chronic impingement can lead to bursal inflammation, tendonitis and can eventually cause degenerative changes and tears of the cuff tendons if not treated (Lin, Weintraub & Aragaki 2008, p. 627; Nho et al. 2008, p. 988).
- The height of the subacromial space, from the head of the humerus to the coracoacromial arch, is only 1.0–1.5 cm as seen on radiographs. Changes of this space occur in subjects with healthy shoulders;
Neer described three stages of impingement
| Stage 1 | Stage 2 | Stage3 | |
| Age | Less than 25 | 25-40 | More than 40 |
| Signs: | Swelling or redness | Tendinitis/bursitis | Bone spurs, tendon tears. |
| Symptoms | Sub acromial pain
Tenderness Painful arc Muscles are strong but painful |
Range of motion restriction in capsular pattern | Weakness in movements like abduction and external rotation
Squaring of acromion |
| Treatment | Reduce pain
Swelling Proximal control exercises |
Work on improving range of motion | Based on the tear. |
SIGNS AND SYMPTOMS:-
- Although impingement symptoms may arise following trauma,
- The pain more typically develops insidiously over a period of weeks to months.
- The pain is typically localized to the front or side of the tip of the shoulder and radiates to till the mid portion of the arm.
- Patients experience pain at night, exacerbated by lying on the involved shoulder, or sleeping with the arm overhead.
- Normal daily activities such as combing one’s hair or reaching up into a cupboard become painful.
- Weakness and stiffness may also be encountered, but they are usually secondary to pain.2
EXAMINATION:-
A thorough physiotherapy objective examination includes:-

- Testing of the neck including ROM, palpation and provocation tests are done to rule out referred pain.
- The shoulder girdle is examined for atrophy, weakness and for shoulder blade and arm muscles asymmetry
- Active and passive shoulder ROM is assessed (where in we find that limited Active shoulder movements but passive movements are full
- strength in all planes is tested once the pain is in control.
- Tests for impingement and instability are performed, as well as a detailed neurovascular assessment is done.
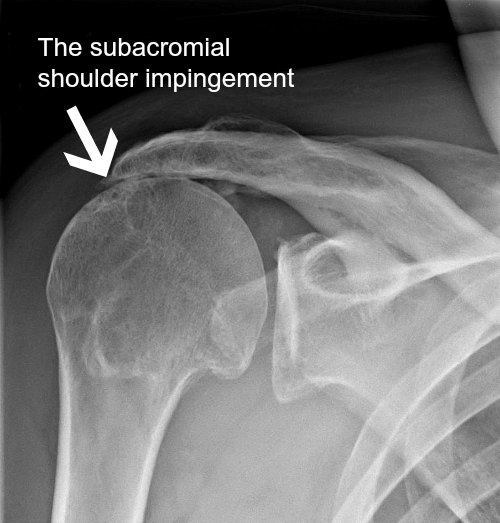
INVESTIGATIONS:-
X-ray:- On an X-ray a loss of subacromial space may be seen indicating of SAIS, but it should not be used solely for diagnosing SAIS.
Other imagings used are US and MRI.

Presence of a tear on MRI does not necessarily correlates with symptoms, especially in the older population (Matava, Purcell & Rudzki 2005, p. 1411).
MANAGEMENT:-
There is no one recipe for treating this kind of shoulder pain. Systematic Research on Exercises and manual therapy effects in Impingemnt says:-
- Exercises are effective in reducing pain (also stated by Senbursa, Baltaci & Atay 2007, p. 920; Trampas & Kitsios 2006, p. 125; Michener, Walsworth & Burnet 2004, p. 163)
- Home exercise is effective as supervised exercise.

- May be better effect if combined with manual therapy (also stated by DeSantis & Hasson 2006, p. 78; Trampas & Kitsios 2006, p. 127; Faber et al. 2006, p. 21; Senbursa, Baltaci & Atay 2007, p. 915; Michener, Walsworth & Burnet 2004, p. 162).
- Acromioplasty with postoperative exercise can improve symptoms.
- Functional shoulder brace may be effective in reducing pain and increase strength.
- Faber et al. (2006, p. 21) found that combination of exercise and manual therapy is most effective in improving function.
- Senbursa, Baltaci & Atay (2007, p. 915) found that improvement in function, strength and decrease in pain is significantly higher with manual therapy compare with self-training in patients with impingement syndrome. Combining manual therapy with supervised exercise may be even more beneficial (Senbursa, Baltaci & Atay 2007, p. 920).
- DeSantis and Hasson (2006, p. 86) found that MWM might be effective as a treatment for patients with SAIS in improving function, AROM and decreasing pain.
- The findings challenge the belief that posture and its concomitant muscle imbalance comprise an etiologic factor in SAIS’ (Lewis, Green & Wright 2005, p. 385).
- Kibler (2006, p. 42) states that there is clear link between impingement and scapular dyskinesis and thus must be addressed.


- Lewis, Wright and Green (2005, p. 72) found that correcting posture (scapula + thorax) with taping, increase Flexion and Abduction ROM and delayed the point at which pain was first experienced, but didn’t change pain intensity. The purpose of the tape was to extend the thoracic spine, and retract, depress and posteriorly tilt the scapula (Lewis, Wright & Green 2005, p. 82).
- Multiple SR (Green, Buchbinder & Hetrick 2003; Michener, Walsworth & Burnet 2004; Van Der Heijden 1997 cited in Kuhn 2009, p. 155) concluded that using US is of minor value in the treatment of shoulder pain; therefore using US is of no value for treating impingement syndrome.
- ‘There is no data for or against the use of cold or heat as a modality; thus, their use must be optional at this point’ (Kuhn 2009, p. 155).
- Cumpston et al. (2007, p. 1-2) in their SR concluded that there is some evidence that glyceryl trinitrate patches are more effective than placebo in the short term (first week of symptoms), and not clear on the long term effect. In addition, headaches were found to be common side effect in one of the studies. There is insufficient evidence to assess its effectiveness in treating rotator cuff disease (Cumpston et al, 2007, p. 15).
- Faber et al. (2006, p. 7) in their SR found conflicting evidence regarding improvement in function after steroid and analgesic injections.
- Regarding functional limitations a SR from 2006 reported ‘strong evidence that extracorporeal shock wave therapy (ESWT) is no more effective than placebo’ (Schmitt et al. 2001; Schmitt et al. 2002; Speed et al. 2002 cited in Faber et al. 2006, p. 21).
- Bal et al. (2009, p. 31) showed that there is no distinct advantage of using low level laser therapy (LLLT) in combination with 12 weeks home exercise program compare to exercise alone, in relation to pain and function among people with SAIS.
- Faber et al. (2006, p.21) in their SR found that laser is not superior to placebo in regard to functional limitations.
- CT evaluated the effectiveness of PEMF in the acute phase of SAIS, found that there isn’t additional benefit to PEMF in that stage (Aktas, Akgun & Cakmak 2007, p. 1234).
- They also found that patients that treated by both nerve block and standard rehab ( ice, pendulum, electrical stimulation, accessory joint play, strengthening, stretches etc) reported significantly less pain during physiotherapy sessions and had better final results compare with standard therapy alone.
These 20 points on various types of treatments preferred for SA impingement or RC impingement are based on systematic research studies and are usually followed at our Physiocure once the patient is examined and diagnosed correctly.
CONCLUSSION:-
Rotator cuff disorders and subacromial impingement are well connected and can predispose to one another. Many theories have been suggested to try and explain the pathoaetiology of these disorders, but it is still a mystery to some extent. To date there is still a debate whether the cause is more due to extrinsic or intrinsic mechanisms, but it seems that the intrinsic theory is gaining momentum in recent years.
Regarding management, there are many tools that can be used; none of them is a “gold standard” treatment and most of them are lacking clear clinical benefit. However, it seems that combination of treatments including some “fancy” manual therapy techniques can contribute to cope with the challenge of treating this pathology.
Finally, if conservative approach has failed, surgical treatment can be considered.
REFERENCES:-
- Aktas, I, Akgun, K & Cakmak, B 2007, ‘Therapeutic effect of pulsed electromagnetic field in conservative treatment of subacromial impingement syndrome’, Clinical Rheumatology, 26, pp. 1234-39.
- Bal, A, Eksioglu, E, Gurcay, E, Gulec, B, Karaahmet, O & Cakci, A 2009, ‘Low-level laser therapy in subacromial impingement syndrome’, Photomedicine and Laser Surgery, 27, no. 1, pp. 31-6.
- Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. Cochrane Database of Systematic Reviews 2003, Issue 1. Art. No.: CD004016. DOI: 10.1002/14651858.CD004016.
- Cleland, J 2007, Orthopeadic Clinical Examination: an evidence based approach for physical therapists, Saunders, Philadelphia, USA.
- Codsi, MJ 2007, ‘The painful shoulder: When to inject and when to refer’, Cleveland Clinic Journal of Medicine, 74, no. 7, pp. 473-88.
- Coghlan JA, Buchbinder R, Green S, Johnston RV, Bell SN. Surgery for rotator cuff disease. Cochrane Database of Systematic Reviews 2008, Issue 1. Art. No.: CD005619. DOI: 10.1002/14651858.CD005619.pub2.
- DeSantis, L & Hasson, SM 2006, ‘Use of Mobilization with Movement in the Treatment of a patient with Subacromial Impingement: A Case Report’, The Journal of Manual & Manipulative Therapy, vol. 14, no. 2, pp. 77-87
- Dorrestijn, O, Stevens, M, Winters, JC, van der Meer, K & Diercks, RL 2009, ‘Conservative or surgical treatment for subacromial impingement syndrome? A systematic review’, Journal of Shoulder and Elbow Surgery, 18, no. 4, pp. 652-60.
- Faber, E, Kuiper, JI, Burdorf, A, Miedema, HS & Verhaar, JAN 2006, ‘Treatment of Impingement Syndrome: A Systematic Review of the Effects on Functional Limitations and Return to Work’, Journal of Occupational Rehabilitation, 16, no. 1, pp. 7-25.
- Haahr, JP & Andersen, JH 2006, ‘Exercises may be as efficient as subacromial decompression in patients with subacromial stage II impingement: 4-8 years’ follow-up in a prospective, randomized study’, Scandinavian Journal of Rheumatology, 35, no. 3, pp. 224-8.
- Kibler, WB 2006, ‘Scapular Involvement in Impingement: Signs and Symptoms’, Instructional course lectures, 55, pp. 35-43.
- Lewis, JS 2009a, ‘Rotator cuff tendinopathy’, British Journal of Sports Medicine, vol. 43, pp. 236-41.
- Lewis, JS 2009b, ‘Rotator cuff tendinopathy/subacromial impingement syndrome: is it time for a new method of assessment?’, British Journal of Sports Medicine, vol. 43, pp. 259-64.
- Lewis, JS, Wright, C & Green, A 2005, ‘Subacromial Impingement Syndrome: The Effect of Changing Posture on Shoulder Range of Movement’, Journal of Orthopaedic & Sports Physical Therapy, 35, no. 2, pp. 72-87.
- Michener, LA, McClure, PW & Karduna, AR 2003, ‘Anatomical and biomechanical mechanisms of subacromial impingement syndrome’, Clinical Biomechanics, 18, pp. 369-79.
- Michener, LA, Walsworth, MK & Burnet, EN 2004, ‘Effectiveness of Rehabilitation for Patients with Subacromial Impingement syndrome: A Systematic Review’, Journal of Hand Therapy, vol. 17, no. 2, pp. 152-64.
- Senbursa, G, Baltaci, G & Atay, A 2007, Comparison of conservative treatment with and without manual physical therapy for patients with shoulder impingement syndrome: a prospective, randomized clinical trial’, Knee Surgery, Sports Traumatology, Arthroscopy, 15, no. 7, pp. 915-21.
- Trampas, A & Kitsios, A 2006, ‘Exercise and Manual Therapy for the Treatment of Impingement Syndrome of the Shoulder: A Systematic Review’, Physical Therapy Reviews, vol. 11, pp. 125-42.